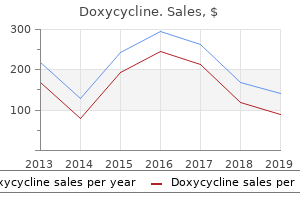
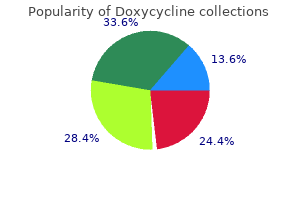
"Purchase doxycycline online pills, antibiotic eye drops pregnancy".
By: T. Ali, M.S., Ph.D.
Co-Director, Ponce School of Medicine
Gitelman syndrome results from genetic abnormalities in the proteins involved in distal convoluted tubule sodium and potassium transport antimicrobial 8536 buy line doxycycline. Liddle syndrome is characterized by severe hypertension antimicrobial silver buy generic doxycycline online, hypokalemia and suppressed renin and aldosterone levels antimicrobial guide doxycycline 100 mg discount. In each case, the increased distal tubular bicarbonate delivery increases potassium secretion. The nephrologist should first consider the possibility of either pseudohypokalemia or potassium redistribution from the extracellular to the intracellular space. Insulin, aldosterone, and its synthetic analogue, fludrocortisone, and sympathomimetic agents such as theophylline and 2-adrenoceptor agonists are common causes of potassium redistribution. In the hypertensive patient, frank hypokalemia in the absence of diuretic use or substantial hypokalemia with diuretic use should suggest primary aldosteronism. Renal potassium loss is most frequently caused by diuretics or metabolic alkalosis. Hypomagnesemia-induced hypokalemia causes renal potassium wasting and is frequently a complication of diuretic use. Rarer causes of renal potassium loss include renal tubular acidosis, diabetic ketoacidosis, and ureterosigmoidostomy. Primary aldosteronism, surreptitious diuretic use or vomiting, concomitant magnesium depletion, and Bartter or Gitelman syndrome should be considered when the cause of the hypokalemia is not obvious. Occasionally, patients are reluctant to admit to self-induced diarrhea, and the diagnosis may need to be confirmed by sigmoidoscopy or direct testing of the stool for cathartic agents. Diagnostic Evaluation Treatment As with any condition, the risks associated with untreated or slowly treated hypokalemia must be balanced against the risks of therapy. Usually, the primary short-term risks are cardiovascular arrhythmias and neuromuscular weakness. Overaggressive therapy can cause acute hyperkalemia, which can cause ventricular fibrillation and sudden death. Close, continuous monitoring of the serum [K+] and the electrocardiogram are necessary to reduce the risk of potentially lethal acute hyperkalemia. In the great majority of hypokalemic patients, emergency therapy is not necessary, and instead a slower approach to replacing the potassium deficit is appropriate. In doing so, it is important to recognize that the amount of potassium required may be much greater than predicted from the deficit in serum potassium concentration. This reflects several factors, most prominently gut sensors that minimize changes in serum potassium levels. If patients with diuretic-induced hypokalemia require ongoing diuretic administration, addition of potassium-sparing diuretics may be considered. Hypomagnesemia can lead to refractoriness to potassium replacement because of inability of the kidneys to decrease potassium excretion. Progressive hyperkalemia results in identifiable changes in the electrocardiogram. This low frequency is a testament to the potent renal mechanisms for potassium excretion. Accordingly, hyperkalemia should suggest an underlying impairment of renal potassium excretion. Rarely, pseudohyperkalemia or a condition that shifts potassium from intracellular to extracellular space is present. Hyperkalemia can be asymptomatic, can cause mild symptoms, or can be life threatening. The initial effect of hyperkalemia is a generalized increase in the height of the T waves, most evident in the precordial leads, but typically present in all leads, which is known as "tenting. Skeletal muscle cells are particularly sensitive to hyperkalemia, causing weakness ("rubbery" or "spaghetti" legs).
Figures are not given for percentages reabsorbed or remaining in every region because quantitative information is incomplete antibiotics dogs cheap 100mg doxycycline mastercard, but most filtered potassium is reabsorbed in the proximal convoluted tubule and thick ascending limb of Henle; approximately 10% of the filtered load reaches the early distal tubule virus 1999 torrent generic 200 mg doxycycline overnight delivery. However virus structure discount 100 mg doxycycline overnight delivery, an intrinsic feature of tubular function is that the extent of Na+ reabsorption in a given nephron segment is about proportional to the Na+ delivery to that segment. Most studies have focused on the proximal tubule because glomerulotubular balance by this segment serves to stabilize delivery of Na+ and fluid to the distal nephron, permitting efficient secretion of K+ and H+. However, Na+ reabsorption in the thick limb of Henle and distal tubule is also delivery dependent. This partly explains why diuretics acting on the proximal tubule are relatively ineffective compared with those acting more distally. With distal-acting diuretics, there is less scope further downstream for compensatory Na+ reabsorption. This also explains why combining two diuretics (acting at different nephron sites) causes a more striking diuresis and natriuresis. In the proximal tubule, physical factors (Starling forces) operating across peritubular capillary walls may be involved. Glomerular filtration of an essentially protein-free fluid means that the plasma leaving the glomeruli in efferent arterioles and supplying the peritubular capillaries has a relatively high oncotic pressure, favoring reabsorption of fluid from the proximal tubules. Peritubular capillary oncotic pressure would also be reduced, and the tendency of the peritubular vasculature to take up fluid reabsorbed from the proximal tubule would be diminished. Backflux of this fluid is thought to occur through the (leaky) tight junctions, reducing net reabsorption. Although the renal sympathetic nerves and certain hormones can influence reabsorption in the proximal tubule and loop of Henle, under normal circumstances the combined effects of autoregulation and glomerulotubular balance ensure that a relatively constant load of glomerular filtrate is delivered to the distal tubule. It is the final segments of the nephron that exert normal day-to-day control of Na+ excretion. Influence of peritubular capillary oncotic pressure on net reabsorption in proximal tubules. Uptake of reabsorbate into peritubular capillaries is determined by the balance of hydrostatic and oncotic pressures across the capillary wall. Compared with those in systemic capillaries, the peritubular capillary hydrostatic (Ppc) and oncotic (pc) pressures are low and high, respectively, so that uptake of proximal tubular reabsorbate into the capillaries is favored. If peritubular capillary oncotic pressure decreases (or hydrostatic pressure increases), less fluid is taken up, interstitial pressure increases, and more fluid may leak back into the lumen paracellularly; net reabsorption in proximal tubules would therefore be reduced. This stimulates Na+ uptake and further depolarizes the apical membrane, thereby facilitating K+ secretion in the late distal tubule/cortical collecting duct. The mineralocorticoid receptors have equal affinity in vitro for aldosterone and other adrenal corticosteroids, such as cortisol. The circulating concentrations of cortisol vastly exceed those of aldosterone, but in vivo the mineralocorticoid receptors show specificity for aldosterone because of the presence along the distal nephron of the enzyme 11-hydroxysteroid dehydrogenase 2, which inactivates cortisol in the vicinity of the receptor. As indicated in Chapter 1, the loops of Henle of superficial nephrons turn at the junction between outer and inner medulla, whereas those of deep nephrons (long-looped nephrons) penetrate the inner medulla to varying degrees. Evidence suggests that the thin descending limb of superficial nephrons is relatively impermeable to water. This "recycling" of K+ into the tubular lumen is necessary for normal operation of the Na+-2Cl-K+ cotransporter because the availability of K+ is a limiting factor for the transporter (K+ concentration in tubular fluid is much lower than Na+ and Cl-). The U-shaped arrangement of the loop of Henle, in which flow in the ascending limb is in the opposite direction to that in the descending limb, multiplies the single effect to generate a much larger vertical (corticomedullary) osmotic gradient by a process called countercurrent multiplication. Fluid entering the descending limb from the proximal tubule is isotonic (~290 mOsm/ Transport Mechanisms in the Thick Ascending Limb Lumen Cells of thick ascending limb Interstitial fluid Na+ K+ K+ 2Cl- Na+ K+ K+ K+ Cl- Cl- Na+ H+ Na+ K+ Ca2+ Mg2+ + Lumen-positive potential difference Paracellular diffusion Figure 2-10 Transport mechanisms in the thick ascending limb of Henle. The transepithelial potential difference drives paracellular transport of Na+, K+, Ca2+, and Mg2+.
Order 100mg doxycycline amex. TTIP and Antimicrobial Resistance.
During filling antibiotics for uti in pregnancy buy doxycycline toronto, the first desire to void is normally at a detrusor pressure of less than 10 cm H2O treatment for glaucoma dogs cheap doxycycline 100 mg online. The voiding pressure should normally be less than 40 cm H2O (and is lower in women) antibiotics for dogs wounds doxycycline 200 mg generic. Detrusor instability is an unstable (spontaneous) contraction occurring with a detrusor pressure above 15 cm H2O. In combination with radiologic imaging (videocystometrography), the following are recorded: bladder neck, closed or open; bladder pressure, end filling; voiding detrusor pressure; bladder stability; compliance; flow rate, maximum; sensation, first; volume, voided and residual. Unfortunately, 95% of patients have sphincter dyssynergia (inability to relax urethral sphincter), which results in no relaxation and incomplete emptying of the bladder. Patients with incomplete lesions may have some control of the distal sphincter and normal anal and sacral reflexes. Ironically, although this latter group has the least neurologic deficit, they have the worst bladder situation, generating high pressures and great risk for renal injury. These intermediate bladders are poorly compliant, and patients have no voluntary control of their sphincters. Natural History Acontractile Behavior About 25% of patients have no detrusor activity, and the bladder overflows when it is sufficiently full. About 14% of patients have renal complications at birth and are at high risk in the next few years. Ultimately, about 52% will develop upper tract problems, although these can take up to 30 years to occur. In one prospective study, renal outcome could be predicted by the urodynamic findings, with worst outcomes related to increased bladder wall thickness, degree of reflux, urethral pressures above 70 cm H2O, and reduced bladder capacity. Meningocele implies that the meninges extend beyond the confines of the vertebral canal with no neural elements contained inside. Spinal dysraphism (symptomatic spina bifida occulta) defines a group of structural anomalies of the caudal end of the spinal cord that do not result in an open vertebral canal but are associated with incomplete fusion of the posterior vertebral arches. Sacral agenesis is a rare anomaly in which part or all of two or more vertebral bodies is absent. It occurs early in fetal development when there is failure of ossification of the lowest vertebral segments. Pathogenesis the neural tube normally forms as the neural folds close over and fuse, starting in the cervical region and progressing caudally. It is believed that the embryologic defect is an incomplete tubularization of the neural tube, with inadequate mesodermal invagination and subsequent arrest of vertebral arch formation. The incidence of myelodysplasia varies from 1 to 5 in 1000 live births, but there are wide geographic variations. Monozygotic twins are often discordant for spina bifida, but siblings are at increased risk (1: 10 to 1: 20), and children of affected parents have a 4% chance of having a similarly affected child. Folic acid supplements taken during the last trimester reduce the incidence of myelodysplasia by 52%. During development, some children develop progressive neurologic disturbance with bladder dysfunction, bowel dysfunction, scoliosis, and a syndrome of pes cavus and limb growth failure. Bladder Dysfunction Neuropathic bladder can be an isolated problem with abnormal urodynamic studies but a normal neurologic examination. The antegrade continent enterostomy procedure has been developed to improve the management.
In affected individuals over 5 years of age antibiotic resistance china buy 200 mg doxycycline with visa, the most common skin lesions are facial angiofibromas antibiotic knee spacers buy on line doxycycline. Angiomyolipomas rarely occur before 5 years antibiotics for nasal sinus infection 200 mg doxycycline overnight delivery, but increase in frequency and size with age. Lymph node and splenic involvement likely represent multifocal origin rather than metastases. Clinical manifestations result from hemorrhage (intratumoral or retroperitoneal) or mass effects (abdominal or flank masses and tenderness, hypertension, renal impairment). However, as with angiomyolipoma, renal cysts tend to increase in size and number over time. Renal Angiomyolipomas Renal Cysts Renal Neoplasms Figure 47-7 Facial angiofibromas in tuberous sclerosis complex. The angiofibromas are small red bumps giving a facial rash in a butterfly distribution and on the chin. A, Cut section shows multiple angiomyolipomas in kidney of 60-year-old symptomatic woman. Treatment Tuberous sclerosis complex is a pleiotropic disease in which the size, number, and location of the lesions can be variable, even among affected individuals within the same family. Major and minor criteria have been developed to guide the diagnostic approach (Box 47-1). The median age at presentation for both renal cysts and angiomyolipoma is 10 years, although these lesions have been detected in infancy. Historically, ultrasound screening has been the preferred modality because it does not involve radiation, is fast and relatively inexpensive, and has high sensitivity in detecting the fat-rich angiomyolipomas and renal cysts. However, given the potential for growth and associated complications, such as pain, bleeding, and hypertension, annual imaging is recommended. Larger angiomyolipomas frequently develop microaneurysms and macroaneurysms, and the risk of serious hemorrhage correlates with aneurysms over 5 mm in diameter. When an associated malignancy cannot be excluded, renal-sparing surgery is preferred, such as enucleation or partial nephrectomy. The increased frequency and size of the angiomyolipomas in women and the reports of hemorrhagic complications during pregnancy suggest that female sex hormones may accelerate the growth of these lesions. Therefore, it is prudent to caution patients with multiple angiomyolipomas about the potential risks of pregnancy and estrogen administration. Surgical decompression of cystic kidneys has been suggested, but no significant beneficial effect has been established. This transcriptional dysregulation promotes the pathologic growth and survival of endothelial cells, pericytes, and stromal cells and ultimately their malignant transformation. The mean age of symptomatic presentation is 35 to 40 years, although patients have been diagnosed in adolescence. Deterioration of renal function caused by cystic kidney disease has been reported but is unusual. Tuberous sclerosis complex should be considered in the differential diagnosis of multiple renal tumors. Focal tubular obstruction and renal parenchymal ischemia have both been suggested as etiologic processes.